CHAMPIONS was a 10-year open-label, prospective follow-up of the pivotal phase 3 CHAMPS study (Study 2) and the CHAMPIONS 5-year follow-up.
In the CHAMPIONS prospective 10-year follow-up study, patients randomly assigned in CHAMPS to receive 30 mcg of IM interferon beta-1a once a week were characterized as the immediate treatment (IT) group (n=81), and those randomly assigned to receive placebo were characterized as the delayed treatment (DT) group (n=74).
For the IT group, treatment with AVONEX was initiated early, that is, within a month after onset of clinically isolated syndrome (CIS), and for the DT group treatment was initiated a median of 30 months (interquartile range, 24-35 months) after CHAMPS randomization.
All patients were offered, but not required, to take 30 mcg of IM interferon beta-1a once a week at enrollment. All MS-related disease-modifying therapies (DMTs) and symptomatic therapies (with the exclusion of investigational therapies) were prescribed at the discretion of the study investigator and in accordance with local practices.
aAlternative (other) therapies included SC interferon beta-1b and interferon beta-1a, glatiramer acetate, intervals of high-dose corticosteroid treatment, mitoxantrone hydrochloride, and natalizumab.
Study limitations
The study was an open-label extension study
Long-term study design includes the possibility of selective attrition of patients with greater levels of disease activity
The study protocol did not include the measurement of neutralizing antibodies against interferon beta
At the end of the study, individual patients (n=10 of 127) may no longer have met the criteria for relapsing MS based on retrospective assessment
As with all sampling, there is a possibility of significant nonrandom differences between cohorts. The CHAMPIONS 10-year cohort reflects a sampling of the CHAMPIONS 5-year cohort, which in turn was only a sampling of the original CHAMPS cohort
Further studies are needed to determine whether there are particular high-risk groups that require immediate initiation of DMTs
Disclosure
CHAMPIONS was funded by Biogen.
CHAMPIONS 10-year extension results2
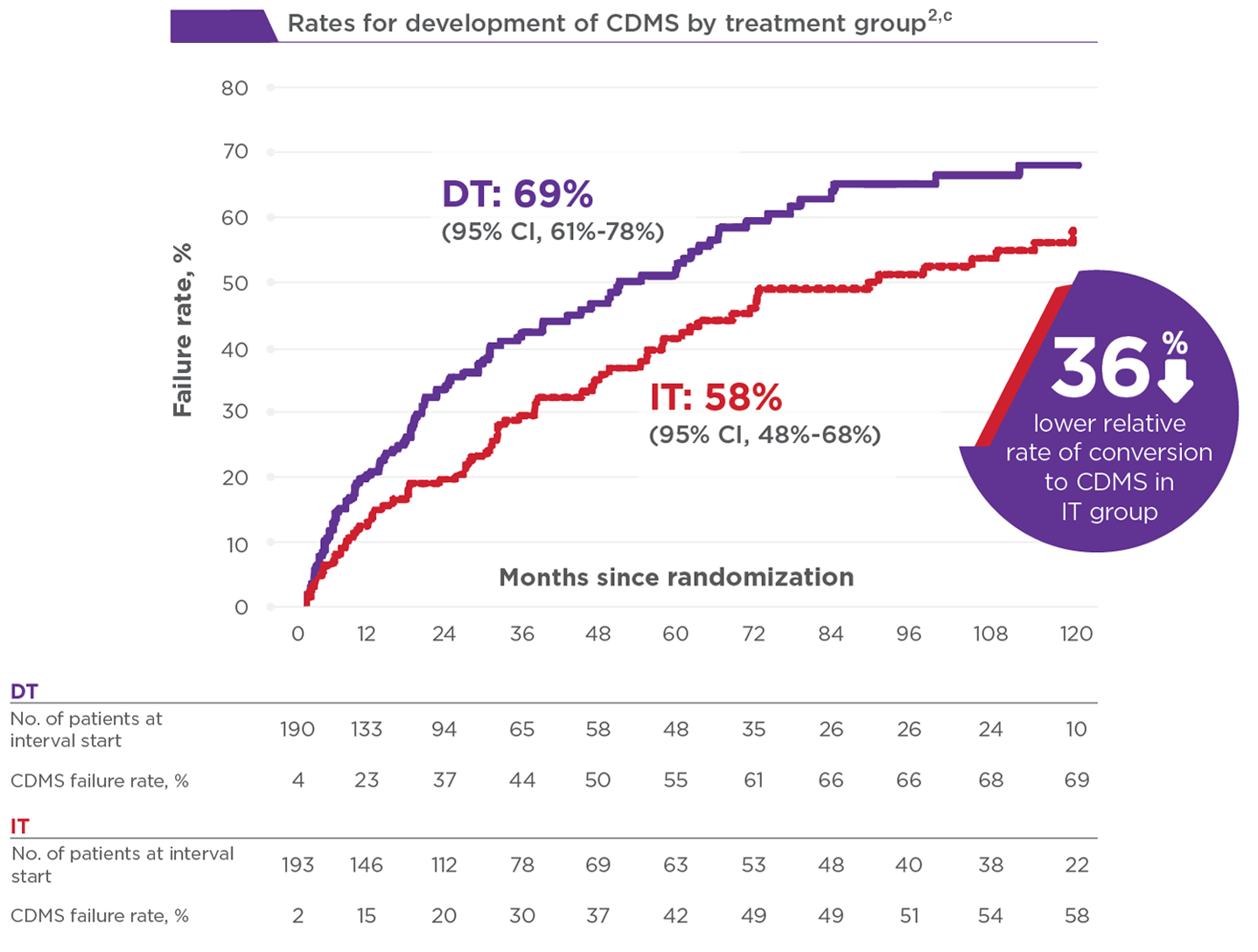
Early treatment with AVONEX reduced rate of progression to CDMS at 10 years
At 10 years, the cumulative probability of developing clinically definite multiple sclerosis (CDMS)b was significantly lower in the IT group (58% [95% CI, 48%-68%]) than the DT group (69% [95% CI, 61%-78%]) (unadjusted hazard ratio, 0.64 [95% CI, 0.48-0.87]; P=0.004). The treatment effect was comparable when adjusting for age, CHAMPS qualifying event, number of CHAMPS baseline T2 lesions, and baseline number of Gd+ lesions (adjusted hazard ratio, 0.61 [95% CI, 0.45-0.82]; P=0.001).
bDefined as development of a second exacerbation in an anatomically distinct region of the central nervous system in patients with CIS.
cKaplan-Meier rates for the development of CDMS calculated using timing from the first month. Patients not meeting the criteria for CDMS were censored on the date of their last neurologic examination.
81% (103 of 127) of patients had an EDSS score below 3.0 at 10 years2
9% (n=12) of all patients and 16% of CDMS patients reached an EDSS score of 4.0 or greater
6% (n=7) of all patients and 10% of CDMS patients reached an EDSS score of 6.0 or greater
Additional efficacy results2
Annualized relapse rate (ARR) in the DT group was double that of the IT group from years 5 to 10 (0.31 vs 0.14; P=0.03), even though use of interferon beta-1a was comparable during that time. A similar trend was observed during the first 5 years (0.36 vs 0.18; P=0.04) and over the entire 10 years (0.33 vs 0.16; P=0.02), but these differences did not meet the 0.01 threshold for statistical significance
There were no significant differences between the IT and DT groups for any of the MRI measures conducted in the study
56% (45 of 81) of patients who started on AVONEX (IT group) were on AVONEX 10 years later3
Discover ASSURANCE, a 15-year follow-up of the MSCRG pivotal trial5
ASSURANCE, a multicenter, observational, single-time-point evaluation of patients conducted 15 years after the MSCRG pivotal trial (Study 1), evaluated the impact of AVONEX treatment on long-term disability in patients who completed 2 years in the MSCRG study.
The primary endpoints of ASSURANCE were change in EDSS score from baseline (start of MSCRG study) and percentage of patients with EDSS scores of at least 4, at least 6, and at least 7. Physician-measured EDSS scores were obtained during the original MSCRG study. Patient-reported EDSS scores were used for the 15-year time point.
In the ASSURANCE 15-year follow-up study, patients were eligible regardless of current treatment or treatment assignment in the MSCRG study. Deceased patients were included if they were deceased at the time of the 8-year follow-up and/or if they were listed in a public database as deceased. A total of 172 patients from the MSCRG study were eligible, and 122 living patients (71%) were enrolled in ASSURANCE. An additional 14 patients (8%) were deceased. Thus, we were able to determine the status of 79% (136/172) of the eligible patients. The analysis focused on the 122 living patients.
Propensity scores were calculated to estimate the probability of current AVONEX treatment given the observed baseline covariates. Propensity score analysis is a rigorous statistical technique used in observational studies to correct for any measured baseline differences between nonrandomized groups.
dPatients not currently taking AVONEX were either not on any therapy or were using different medications, including natalizumab, glatiramer acetate, SC interferon beta-1b, SC interferon beta-1a, and methotrexate.
Study limitations
Incomplete ascertainment, a problem inherent in long-term follow-up studies, lowers power and may skew the results because of informative censoring
As no randomization to treatment existed beyond the MSCRG core study, it is assumed that unmeasured factors contributed to treatment decisions during the follow-up interval. While not a replacement for randomization, the use of propensity score weightings results in more equivalent comparison groups
There may be inherent biases in nonrandomized observational studies. Despite the use of propensity score weightings to adjust for baseline differences between comparison groups and to reduce bias that could arise from the lack of randomization in AVONEX use after the 2-year clinical trial, multiple unobserved factors may have influenced the beneficial outcomes for those currently on AVONEX. Such possible biases include the presence of less aggressive disease, better adherence to therapy over time, and better overall health and symptom management
Although these data show that a subgroup of patients do well on AVONEX over the long term, the reason for this result (therapeutic effect vs different natural history) cannot be fully addressed by these data. It is impossible to draw causal inferences between either the continued use of AVONEX or a fundamentally benign natural history in the group of patients with better long-term outcomes
The group of patients described is relatively small and initially was enrolled based on select criteria for disease activity; therefore, extrapolating the results of this study to the entire population without confirmation in additional patient samples is hazardous
Patients continuing to use AVONEX at the 15-year time point were more likely to have been randomized to AVONEX during the clinical trial (38 current users originally randomized to AVONEX vs 18 originally randomized to placebo) and had slightly lower EDSS scores at study entry (2.1±0.77 vs 2.4±0.85)
Presumably, the magnitude of benefit for active versus placebo treatment in this patient sample was not sufficiently large to overcome the effects of small patient numbers and inconsistent treatment patterns over the long follow-up interval
The self-reported EDSS used in this trial has been shown to have a strong correlation between patient and physician reports. As such, we believe that any discrepancies between patient and physician EDSS scores are more than counterbalanced by the higher ascertainment rate possible by the self-report method, particularly at the higher EDSS levels, when patients are less likely able to travel to the site for a physician-derived EDSS
Disclosure
ASSURANCE was supported and funded by Biogen.
ASSURANCE 15-year follow-up study results
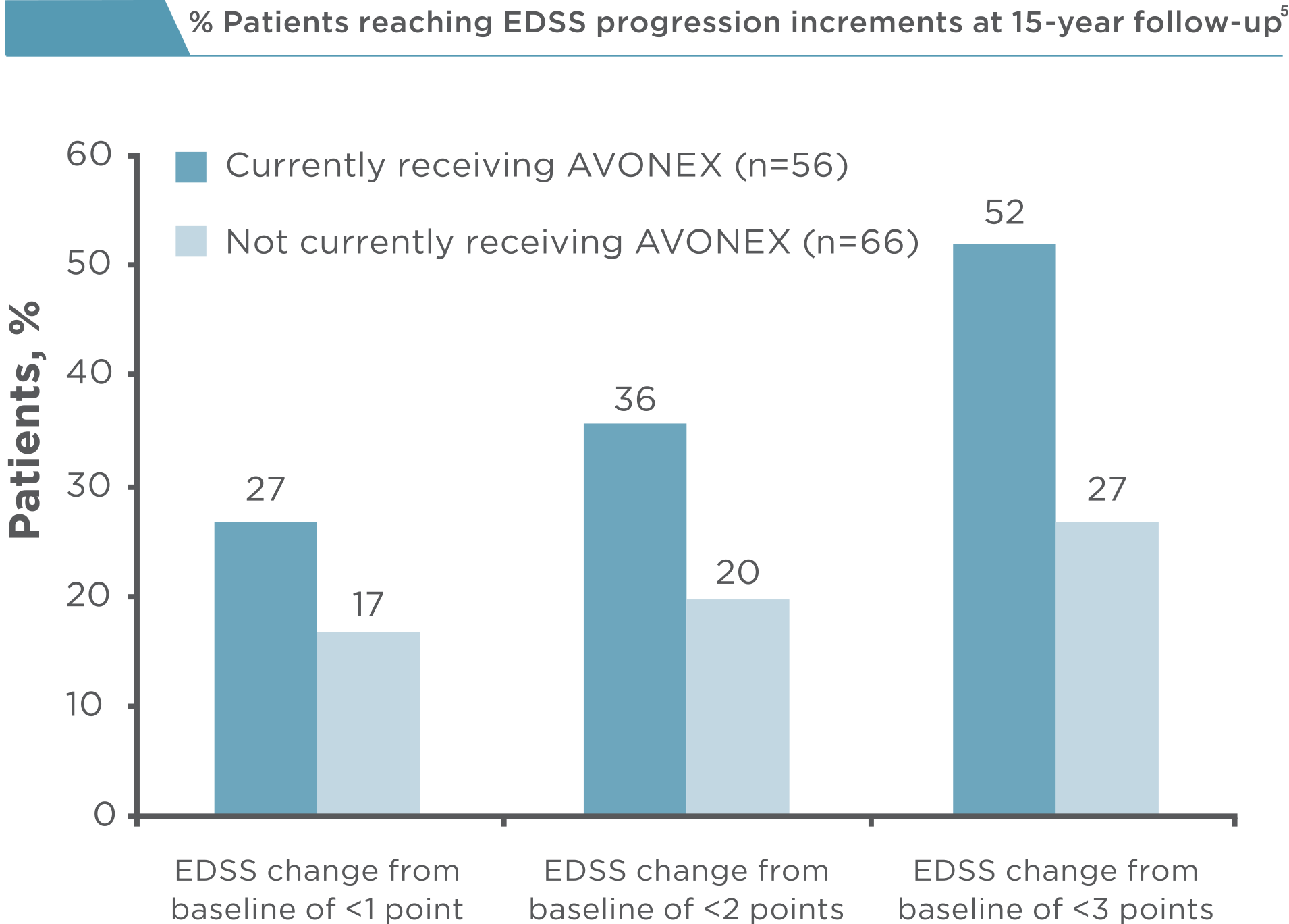
At 15-year follow-up, patients on AVONEX experienced less disability compared with patients not currently taking AVONEX
The mean EDSS score for patients on AVONEX was 4.4 versus 5.7 for patients not on AVONEX (median, 5.0 vs 6.0; range, 0-8.5 vs 0-9.0)
Patients currently on AVONEX had a smaller mean change from baseline EDSS score versus those not currently on AVONEX (2.3 vs 3.3; median, 2.5 vs 4.0; range, –1.5 to 6.5 vs –2.0 to 6.5)
27% of patients currently on AVONEX had a stable disability score since enrollment into the MSCRG trial versus 17% of patients not currently on AVONEX
Patients on AVONEX at 15-year follow-up reported:
64% reached an EDSS milestone of 4.0 versus 83% of patients not on AVONEX
32% reached an EDSS milestone of 6.0 versus 62% of patients not on AVONEX
9% reached an EDSS milestone of 7.0 versus 33% of patients not on AVONEX
Patient use over 15 years
Nearly half the patients enrolled in ASSURANCE were taking AVONEX at
15-year follow-up
46% (56 of 122) of patients were on AVONEX at 15-year follow-up
13.3 years was the median duration of use among patients currently taking AVONEX (mean, 12.1; range, 3-15 years)
Of these 56 patients, 80% used AVONEX for at least 10 years
AVONEX was the only DMT that had been used by 42 of 56 patients (75%) currently on AVONEX